… a small fraction of the population reports a chronic debilitating condition after COVID-19 vaccination, often referred to as post- vaccination syndrome (PVS). To explore potential pathobiological features associated with PVS, we conducted a decentralized, cross-sectional study involving 42 PVS participants and 22 healthy controls enrolled in the Yale LISTEN study. Compared with controls, PVS participants exhibited differences in immune profiles, including reduced circulating memory and effector CD4 T cells (type 1 and type 2) and an increase in TNFα+ CD8 T cells. PVS participants also had lower anti-spike antibody titers, primarily due to fewer vaccine doses. Serological evidence of recent Epstein-Barr virus (EBV) reactivation was observed more frequently in PVS participants. Further, individuals with PVS exhibited elevated levels of circulating spike protein compared to healthy controls. These findings reveal potential immune differences in individuals with PVS that merit further investigation to better understand this condition and inform future research into diagnostic and therapeutic approaches.
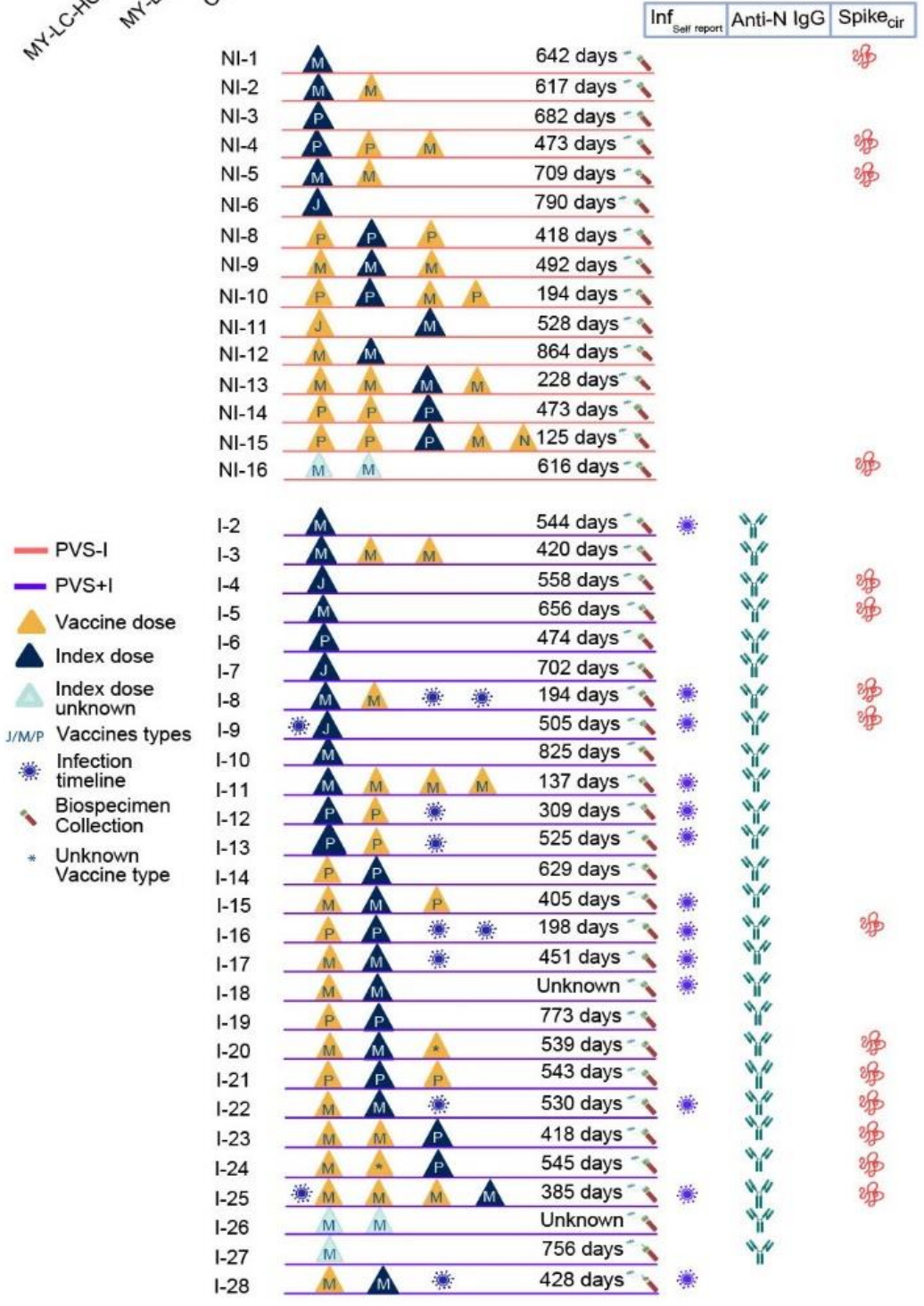
The most striking finding from this study is that circulating Spike protein was detectable up to 709 days after COVID-19 mRNA Injection:
They also found that “participants with PVS had significantly higher circulating S1 levels compared with the control group (p = 0.01).” The study further confirmed that the presence of S1 reflects the presence of full-length (‘vaccine’) Spike protein:
The full-length S SPEAR assays showed a significant correlation between S and S1 across all samples (Fig. 5E), as well as for values above the LLoD and LLoQ (Fig. 5F, Table S2). Thus, based on SPEAR assays, the individuals with PVS exhibited elevated levels of circulating full-length S compared to healthy controls.
This greatly clarifies the situation. Cardiac doses (11,000 FU/d) of nattokinase, and good blood levels of vitamin-D might be of significant benefit to these unfortunate folks.
It's important to note that the McCullough protocol 2 of 3 elements Bromelain and Nattokinase, need to be taken on an empty stomach to be effective for this purpose. Do not take near food. I'd suggest no closer than 2 hours after eating or at least 1/2 hour before eating. Please comment if you have better directions on the timing.
This is copied from his official website today:
The empiric regimen can be continued for 3-12 months or more and be guided by clinical parameters:
- Nattokinase 2000 FU (100) mg orally twice a day without food
- Bromelain 500 mg orally once a day without food
- Curcumin 500 mg orally twice a day (nano, liposomal, or with piperine additive suggested)





This greatly clarifies the situation. Cardiac doses (11,000 FU/d) of nattokinase, and good blood levels of vitamin-D might be of significant benefit to these unfortunate folks.
It's important to note that the McCullough protocol 2 of 3 elements Bromelain and Nattokinase, need to be taken on an empty stomach to be effective for this purpose. Do not take near food. I'd suggest no closer than 2 hours after eating or at least 1/2 hour before eating. Please comment if you have better directions on the timing.
This is copied from his official website today:
The empiric regimen can be continued for 3-12 months or more and be guided by clinical parameters:
- Nattokinase 2000 FU (100) mg orally twice a day without food
- Bromelain 500 mg orally once a day without food
- Curcumin 500 mg orally twice a day (nano, liposomal, or with piperine additive suggested)
To see the official website page - use this link and scroll down a ways: https://www.petermcculloughmd.com/